Getting the bulletproof abs you hear so much about is actually not that hard. The secret is choosing the right exercises and doing that ab workout on a regular basis. Consistency builds greatness.
A flat stomach with visible abs is great for the summer and looking good at the beach, but the actual benefit in training your abs is increased athleticism and a better posture. In the long run this is the real benefit of taking care of your abs. Give this routine a try!!
Author: gym-junkiez-community-content
-

Try this Unorthodox Routine for Bulletproof Abs
-

Old School Biceps Workout for Mass
🏋🏻♀️ 1 ON 1 COACHING WITH ME: https://forms.gle/ca7KbhsRFfU1tPcZ7
🏋🏻♀️ TRAINING PROGRAMS: https://www.damienpatrick.com/collect…
👔 TOTAL ALPHA MERCH: https://www.totalalphabrand.com/ USE CODE: Damien
📱 TRY MY APP-7 DAYS FREE- https://damienpatrick.app/
💊 AMINO ASYLUM: https://aminoasylum.shop/ USE CODE: Damien
🍽️ https://www.flexpromeals.com/ USE CODE: Damien
OLD SCHOOL BICEP WORKOUT FOR MASS
*EZ BAR CLOSE GRIP PREACHER CURLS 3X15,12,10 45-60 SECS REST
*EZ BAR WIDE GRIP PREACHER CURLS 3X15,12,10 45-60 SECS REST
*INCLINE DUMBBELL CURLS 4X15,12,10,8 45-60 SECS REST
*SEATED BARBELL CURLS 3X12,12,10 1 DROP SET: 10/5 45-60 SECS REST
*CABLE ROPE CROSS BODY HAMMER CURLS 3X12,12,10 1 DROP SET: 10/ TO FAILURE 45-60 SECS REST
Drop a clip or a pic in the community feed of your arm session. Train Hard!!!!!!
-
The Difference Between Testosterone Replacement Therapy and Steroid Abuse
Testosterone Replacement Therapy is not even close to the same thing as steroid abuse.
Is testosterone a steroid? Technically yes, but not in the way most people mean. Testosterone is not an illegal steroid and will not cause “roid rage”.
Testosterone is a naturally occurring steroid hormone produced in the body. Its natural role is to promote bone density, produce sperm in the testes, and stimulate lean muscle growth.
Unfortunately, the facts are muddled with myths, rumors, and confusion.

TRT Is Not the Same as Illegal Steroid Abuse
Many people are under the false impression that choosing Testosterone Replacement Therapy (TRT) to normalize testosterone levels will produce exactly the same effects as the extremely high testosterone levels that are associated with abusing steroids.
Many people mistakenly associate TRT with bodybuilding. They fear the possibility of becoming instantly and unnaturally bulky like “that guy” in the gym and of suffering uncontrolled side effects, like liver damage or the development of male breasts.
They’re worried about experiencing uncontrolled aggression, commonly known as “roid rage.”
However, these are misconceptions about TRT that couldn’t be further from the truth.
People are confusing two entirely different things.
TRT is a safe medical treatment for a legitimate medical condition. Using extremely high dosages of testosterone cypionate (commonly used in TRT) in conjunction with other compounds is considered steroid abuse, which is not recommended due to safety concerns.
If anyone chooses to use steroids for muscle growth and/or strength, it is highly recommended that a medical professional monitors health markers closely.What Does Testosterone Do?
Among other roles in your body, testosterone causes an increase in the size of your muscle cells. This means each individual muscle cell will grow.
Because bigger muscles tend to also be stronger, your strength can increase as a result. In turn, increased muscle mass burns more calories, helping to establish and to maintain a better balance between lean muscle and excess body fat.
Balanced levels of testosterone can improve an individual’s sense of emotional wellbeing as well as their concentration and focus, which can improve performance in the mental aspect of work or competition.
TRT and Steroids — What’s the Difference?
If you’re suffering from low testosterone and are experiencing deficiencies in strength, muscle mass, sexual performance, or concentration, restoring normal testosterone levels may help restore performance, including at work, in sports, and in the bedroom.
Obtaining medication illegally and boosting testosterone to extreme levels may lead to artificial muscle gains, an increase in performance at your chosen athletic endeavor, and enhanced performance in the bedroom, but it may also have the opposite effect in those areas (in addition to being dangerous, potentially causing life-long damage to your body, and being illegal).
Thus, we begin to see the differences between the medical treatment known as TRT and the risky and illegal practice of steroid abuse for some competitive edge or cosmetic benefit.
The differences are found in the goals, purpose, amounts, and application.
The Facts About Steroid Abuse
Illegal steroids are abused for cosmetic benefits or physical performance reasons — to build muscle and lose body fat or to enhance one’s ability to perform in a sport or excel in bodybuilding.
Steroid abusers aren’t lacking in endogenous (naturally produced) testosterone, and they’re using supplementary testosterone to cheat natural processes.
The following are important facts about illegal steroid abuse:
- Steroids are often obtained and injected illegally at very high doses.
- This treatment is not approved by the FDA.
- There are no diagnostic tests to determine if someone needs anabolic steroids for recreational purposes.
- A total lack of medical oversight leads to uncontrolled side effects and health risks.
Steroid abusers usually don’t use testosterone only. In addition to huge doses of testosterone, they’re adding other substances on top, some of which may be illegal.
It’s a simple matter. The primary concern with steroid abuse is one of safety. It’s never advised to risk your long-term health for a competitive or cosmetic edge.
The Facts About Testosterone Replacement Therapy (TRT)
Testosterone Replacement Therapy is a medical treatment prescribed and administered by health care professionals to help treat the effects of low testosterone levels in men.
Administration of supplemental testosterone begins only if medically valid diagnostic tests determine there is an actual deficiency in one’s testosterone level.
You generally need to exhibit symptoms of low testosterone and have a total level of testosterone below 300 ng/dL or a free testosterone level below 9.0 ng/dL (for men).
Because low testosterone is a recognized medical condition, your medical care provider can prescribe testosterone to you in a controlled TRT treatment protocol. The goal is to restore levels to an optimum range, not an extreme range.
Properly administered Testosterone Replacement Therapy has a number of potential benefits, including:
- Increased lean muscle production and strength
- Reduced fat tissue production
- Improved erectile function
- Increased sexual desire (libido)
- Improved mood and increased sense of well-being
- Reduced anxiety and improved concentration
- Increased energy and motivation
These benefits are accessible to patients following a monitored treatment protocol without all the countless and unpredictable side effects of steroids abuse.
These benefits might help an athlete to improve their performance on the field to a small degree, but your body will not change to the unnatural degree it would when abusing steroids without proper supervision.

Steroid Abuse and TRT: Side Effects Are Different
Some of the side effects that can be caused by TRT include:
- Acne
- Slight male breast development
- Enlarged prostate
- Difficulty urinating
- Mood swings
- Fluid retention
When you’re being treated with medically indicated Testosterone Replacement Therapy, we’re monitoring your health, and we’re making very sure you aren’t given a dose that’s too high or too low. We know how to minimize these side effects or prevent them all together.
Some of these same side effects can occur with steroid abuse, but their severity is much more pronounced due to the unnatural hormone levels reached when abusing testosterone. Other side effects of illegal steroid use are flat-out dangerous:
- Large male breast development
- Disease of the liver or spleen
- High blood pressure
- Increased cholesterol
- Blood clots
- Heart disease
Testosterone Replacement Therapy can be safe, effective, and side-effect free when provided under the guidance of a trained professional. This makes all the difference.
Making sure that your health is not sacrificed in the name of “higher T levels” is one of the most important roles of a TRT provider.
Learn More About Safe and Effective Treatment for Low T
Understand that any medicine can be a poison; it all depends on the dose and proper medical supervision. Make sure that when you choose someone to help you with your Low T symptoms, you select a provider with the knowledge and expertise to improve your quality of life while also keeping you safe.
-

Full Chest Mass Building Workout
video by Damien Patrick
FULL CHEST MASS BUILDING WORKOUT
HIGH CABLE CHEST PRESS
4X15,15,12,12
60-75 SECS RESTINCLINE BARBELL CHEST PRESS
4X15,12,10,8
75-90 SECS RESTINCLINE DUMBBELL CHEST PRESS
4X12,12,10,10
75-90 SECS RESTFLAT HAMMER STRENGTH CHEST PRESS
4X12,12,10,10
60-75 SECS RESTINCLINE DUMBBELL FLY
4X12,12,10,10
60-75 SECS RESTHIGH CABLE FLY
3X15,12,10
1 DROP SET: 10/ TO FAILURE VERY SLOW NEGATIVE REPS
45-60 SECS REST💪🏻 TRAINING PROGRAMS: https://www.damienpatrick.com/collect…
👕TOTAL ALPHA CLOTHING: https://www.totalalphabrand.com/
💪TRANSFORMATION AND CONTEST PREP COACHING: https://www.damienpatrick.com/collect…
📱 TRY MY APP-7 DAYS FREE- https://damienpatrick.app/
💊https://believesupplements.com/collec… USE CODE: Damien
💪LIFTING ACCESORIES: https://www.snakebitefitness.com USE CODE: Damien
-

7 BEST TRAP EXERCISES FOR BIGGER TRAPS
video by Damien Patrick
The trapezius is a large muscle in your back. It starts at the back of your head and neck, extends across your shoulders, and down the middle of your back, forming a trapezoid. Also known as traps, the trapezius muscles play an important role in posture. They move the shoulders, lift arms out to the side, and protect the neck and spine. You use them when you shrug or pull your shoulders back. Check out these exercise options and add them into your program!
💪🏻 TRAINING PROGRAMS: https://www.damienpatrick.com/collect…
👕TOTAL ALPHA CLOTHING: https://www.totalalphabrand.com/
💪TRANSFORMATION AND CONTEST PREP COACHING: https://www.damienpatrick.com/collect…
📱 TRY MY APP-7 DAYS FREE- https://damienpatrick.app/ 💊https://believesupplements.com/collec…
USE CODE: Damien
💪LIFTING ACCESORIES: https://www.snakebitefitness.com USE CODE: Damien
-

A Few Facts about Women and Weightlifting
Weight Training For Women: The Real Differences
There are no “man exercises” or “woman exercises,” but that doesn’t mean women should train exactly like men. Although women gain relative strength and muscle at virtually the same rate as men (1), there are key differences in how women should train to get the best results.
Here are the general guidelines for women, tailored to the female body. I’ve also provided a sample
workout for women so you can see how these guidelines are used.
1. Women benefit from more volume than men.
Research shows that women can generally do more reps at a given intensity than men. So, it’s reasonable to say that women should generally perform more reps per set than men. However, this can lead to using very light weights for endless reps.
The weight you use on each set is determined by the number of reps you’re doing. Both women and men should choose a load that leaves them unable to perform any more than indicated on the workout program, but without cheating by using momentum.
But, since women have greater muscle endurance than men when using light to medium loads (2), they can benefit from doing an additional set. So, if a generic workout program calls for 3 sets of 8-12 reps, women will generally get better results by adding a fourth set.
Adding an additional set takes advantage of women’s superior muscle endurance while keeping each set’s intensity high enough to create strength adaptations.

2. Women don’t need as much rest between sets.
Women recover faster after a set than men because they’re less fatigable (3). Therefore, women don’t need as much rest between sets as men. This is why many women prefer faster-paced workouts like tri-sets and circuits.
Tri-set training – doing three exercises that hit a different muscle group, performed in series – can be more effective than traditional training. It enables you to rest longer between sets of the same muscle group while maximizing training time by doing a set targeting a different muscle group.
Tri-sets are especially great for women because they allow them to keep moving, which maximizes work while still getting ample rest between sets hitting the same muscle group – important for getting the most out of each set.
3. Women can train their upper bodies more often than men.
Women not only recover faster than men after each set, but they also recover faster after workouts.
For example, one study of males and females involved performing the bench press three times per week for five sets at 50% to 100% of perceived five-rep max (5RM). After the program, the subjects, on three consecutive weeks, participated in two testing sessions per week: baseline session and recovery session. During the testing sessions, subjects performed an estimated 1RM bench press while resting during a 4-hour, 24-hour, or 48-hour recovery period.
Females had no differences in muscle strength, regardless of recovery time, while the males had decreases in estimated 1RM at the 4-hour and 24-hour recovery times. (4)
Interestingly, researchers looking at the bench press and squat performance found no differences between sexes in squats but did find differences in bench press performance.

The difference in upper-body recovery and performance between sexes may be because men generally have 10 times more circulating testosterone than women (5). Upper-body muscles may have more androgen receptors than lower-body muscles (6). So it’s possible that this hormonal difference might permit greater development of upper-body muscles in men compared to women.
What does this mean in practical terms? Women can hit their upper-body lifts more often throughout the week than men. So, if a woman wants to increase her numbers on a certain upper-body lift, she can hit that lift three times per week. (Men should stick to twice per week.)
The same applies to those looking to increase the size of certain upper-body muscles. Women who want bigger shoulders can hit them hard three times per week, while men should train shoulders hard twice per week.
4. Women should do fewer plyometric exercises.
Female bodies use less of the stretch-shortening cycle when it comes to upper-body lifting, which makes them less efficient, slower, and possibly more at risk of injury from explosive plyometric exercises.

The stretch-shortening cycle is more pronounced in men. In several studies, men demonstrated greater stretch-shortening-related power in both lower (7) and upper-body movements. (8,9)
In short, women are better off doing less plyometric volume than men. A simple way to apply this in pre-written workout programs is for women to do one less set than men of jumping, bounding, hopping exercises, or explosive upper-body lifts.
This works out nicely because the ladies can do an extra set of strength training (see number one above) while the guys do an extra set of explosive plyometric exercises.
5. Women can get more from less sprinting.
A study involving male and female soccer players found that men have a superior ability to recover between sprints (10). Males had less drop-off in their sprint speed between subsequent sprints than women.
So, women would do best with fewer rounds of sprints than men in a given workout. Women can do a few extra sets of strength work instead since it’ll likely benefit them more anyway.
6. Women will benefit from more hamstring strength.

Females need to emphasize hamstring-oriented exercises like leaning lunges and RDL lunges. Why? Because women are more quad-dominant than men (11), and they tend to have weaker hamstrings (12), making them more prone to knee injury (13,14).
This doesn’t just mean going bonkers on the RDLs, 45-degree hip extensions, and other exercises that hit your glutes and hams in their lengthened range. It means incorporating some knee flexion exercises, such as machine leg curls and stability-ball leg curls two to three times per week. And anyone trying to build or strengthen hamstrings will need more than one exercise for complete development.
Sample Total-Body Workout for Women
Here’s what a total-body workout for women might look like. This can be done in 60 minutes or less, including a warm-up.
Exercise Sets Reps A1. Squat Jump 3 5 A2. Cable Lateral Raise 3 20-25/side A3. Stability Ball Plate Crunch 3 12-15 B1. Barbell Romanian Deadlift 3 8-12 B2. Side Elbow Plank with Dumbbell Rear-Delt Flye 3 10-12/side B3. Plank with Shoulder Tap 3 20-25 sec. C1. Underhand Grip Lat Pulldown 3 10-12 C2. Dumbbell Behind-The-Head Triceps Extension 3 12-15 C3. NT Loop Glute Walk 3 50 sec. D1. Cable One-Arm Row with Reverse Lunge 3 12-15/side D2. Push-Up 3 max reps D3. Stability-Ball Hamstring Curl 3 15-20 For these tri-sets, perform all reps of an exercise before moving to the next one. Rest no more than 30 seconds between each exercise. Once you’ve completed all three exercises, rest 1 to 2 minutes. Then do the next round.
I’m not saying that men couldn’t benefit from a workout for women or that women wouldn’t benefit from a workout for men. All I’m showing is how I tweak workouts so that women get the most out of their training, given their unique differences.
The workouts I write for women have less explosive work and more strength training. Plus, the workouts I write for men contain more work on the upper traps and arms, whereas the women’s workouts have more work for glutes and hamstrings.
References
by Nick Tumminello
- Gentil P et al. Comparison of upper body strength gains between men and women after 10 weeks of resistance training. PeerJ. 2016 Feb 11;4:e1627. PubMed 3.
- Maughan RJ et al. Endurance capacity of untrained males and females in isometric and dynamic muscular contractions. Eur J Appl Physiol Occup Physiol. 1986;55(4):395-400. PubMed.
- Hunter SK. Sex differences in human fatigability: mechanisms and insight to physiological responses. Acta Physiol (Oxf). 2014 Apr;210(4):768-89. PubMed 1.
- Judge LW et al. The effect of recovery time on strength performance following a high-intensity bench press workout in males and females. Int J Sports Physiol Perform. 2010 Jun;5(2):184-96. PubMed.
- Dreyer HC et al. Resistance exercise increases leg muscle protein synthesis and mTOR signalling independent of sex. Acta Physiol (Oxf). 2010 May;199(1):71-81. PMC 1.
- Kadi F et al. The expression of androgen receptors in human neck and limb muscles: effects of training and self-administration of androgenic-anabolic steroids. Histochem Cell Biol. 2000 Jan;113(1):25-9. PubMed.
- Komi PV et al. EMG activity of the leg extensor muscles with special reference to mechanical efficiency in concentric and eccentric exercise. Int J Sports Med. 1987 Mar;8 Suppl 1:22-9. PubMed.
- Miyaguchi K et al. Gender difference in ability using this stretch-shortening cycle in the upper extremities. J Strength Cond Res. 2009 Jan;23(1):231-6. PubMed 2.
- Flanagan SD et al. The relationship between muscle action and repetition maximum on the squat and bench press in men and women. J Strength Cond Res. 2014 Sep;28(9):2437-42. PubMed.
- Dent JR et al. Sex differences in acute translational repressor 4E-BP1 activity and sprint performance in response to repeated-sprint exercise in team sport athletes. J Sci Med Sport. 2015 Nov;18(6):730-6. PubMed.
- Youdas JW et al. Comparison of hamstring and quadriceps femoris electromyographic activity between men and women during a single-limb squat on both a stable and labile surface. J Strength Cond Res. 2007 Feb;21(1):105-11. PubMed 1.
- Kannus P et al. Peak torque occurrence in the range of motion during isokinetic extension and flexion of the knee. Int J Sports Med. Nov 1993;14(8):422-426. PubMed.
- Anderson AF et al. Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. Am J Sports Med. Jan-Feb 2001;29(1):58-66. PubMed.
- Griffin LY et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. May-Jun 2000;8(3):141-150. PubMed.
-

SHOULDERS AND ARMS WORKOUT FOR MASS
-STANDING LATERAL RAISE
3X15,12,10
1 DROP SET: 10/10
45-60 SECS REST-DUMBBELL SHOULDER PRESS
4X12,12,10,10
60-75 SECS REST-ARNOLD DUMBBELL PRESS
4X12,12,10,10
60-75 SECS REST-CABLE ROPE FACE-PULLS
3X15,12,10
1 DROP SET: 10/10
45-60 SECS RESTSUPERSET
DUMBBELL OVERHEAD EXTENSION
4X12,12,10,10
WIDE GRIP BARBELL CURL
4X12,12,10,10
45-60 SECS RESTSUPERSET
INCLINE EZ BAR SKULL CRUSHER
4X12,12,10,10
CROSS BODY HAMMER CURLS
4X12,12,10,10
45-60 SECS RESTSUPERSET
CABLE EZ BAR MID RANGE CURLS
4X12,12,10,10
CABLE EZ BAR OVERHEAD EXTENSION
4X12,12,10,10
45-60 SECS REST🏋🏽TRY MY WORKOUT APP FOR $1: https://damienpatrick.app/
📱EBOOK PROGRAMS: https://www.damienpatrick.com/collect…
👕TOTAL ALPHA CLOTHING: https://www.totalalphabrand.com/
💪TRANSFORMATION AND CONTEST PREP COACHING: https://www.damienpatrick.com/collect…
💪LIFTING ACCESORIES: https://www.snakebitefitness.com use code: “DAMIEN”
-

The Truth about EPOC (Exercise Afterburn)
by Dr. Jonathan Mike
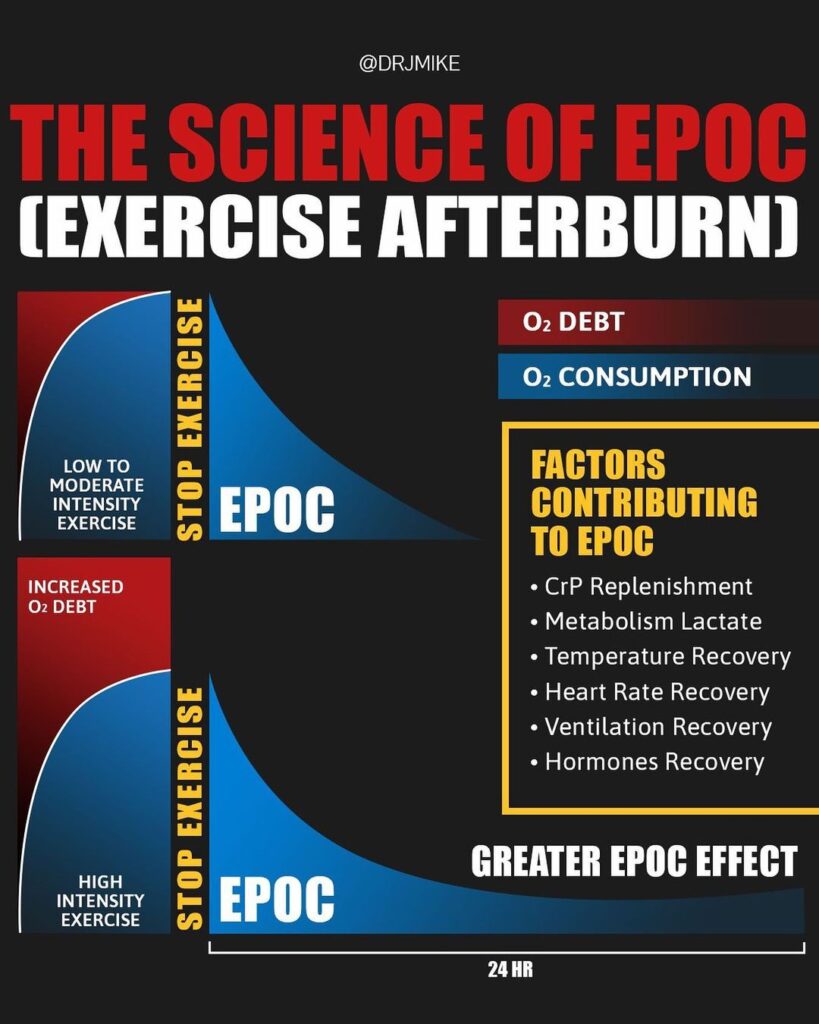
EPOC, technically known as Excess Post-exercise Oxygen Consumption, and more generally known as exercise afterburn, has been widely publicized as an explanation for the benefits of high intensity interval training. It’s the recovery period after exercise where there is elevated oxygen consumption. It’s essentially an elevated metabolic rate after exercise.
The purpose of EPOC is to restore the body to its resting state and create adaptations. The main argument is that if EPOC is greater after high intensity exercise, a greater metabolic rate exists for longer periods of time. By that logic, you would burn more calories leading to greater fat loss. However, this is often overstated.
.
At the start of exercise, the anaerobic energy systems supply the needed ATP for this work. The energy provided during this deficit phase of exercise is employed until a steady state is reached, thus the oxidative system is the dominant energy system being used. Those that are highly trained get to a steady state much quicker vs. untrained.Here’s the real deal
The two biggest factors affecting EPOC are exercise intensity and duration, with intensity being the #1. Some studies have found that EPOC may last up to 72hrs, while others have found it to be much shorter or even a few hours. The large range of EPOC durations is due to differences in exercise intensity, duration and study methods. Despite sensational claims, recent studies conclude that the EPOC effect is fairly small, making only a minor contribution to fat loss. There are also large individual differences in EPOC responses in addition to many factors contributing to EPOC.
.
Take-home messageThose that claim interval training is far superior vs. steady state cardio (or that steady state cardio is bad for you), and use EPOC to back up that claim, they are mistaken. You’ll likely burn the same amount of calories either way. Remember, the biggest driver of fat loss is caloric deficit.
. -

3 Techniques to Build Bigger Muscles
by Damien Patrick
In this video I cover my 3 favorite intensity techniques to help you build bigger muscles. Most people think in order to grow your muscles you must constantly be increasing the weight you use during training. Yes that is definitely important to progress and should be a focus when building muscle but it is not possible to maintain constant strength gain. These tips will help you increase the load you put on the muscles to make them grow without having to increase the weight you use
🏋🏽TRY MY WORKOUT APP FOR $1: https://damienpatrick.app/
📱EBOOK PROGRAMS: https://www.damienpatrick.com/collect…
👕TOTAL ALPHA CLOTHING: https://www.totalalphabrand.com/
💪TRANSFORMATION AND CONTEST PREP COACHING: https://www.damienpatrick.com/collect…
💪LIFTING ACCESORIES: https://www.snakebitefitness.com use code: “DAMIEN”
-
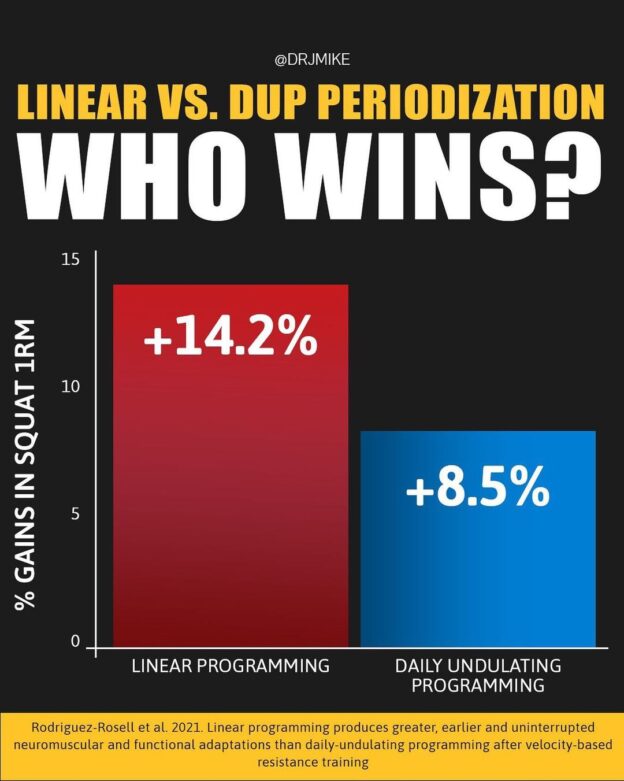
Training Programming- Linear Vs. Dup Periodization- Who Wins?!
by Dr. Jonathan Mike
A lot of people out there love Periodization! Of course linear and DUP (daily undulating) have been around for decades and in the early 2000s DUP/non-linear was thought to be more superior because you could change set, and reps schemes & incorporate within week variations & and add within week recovery. Undulating periodization (also referred to as Non-Linear Periodization) involves varying the stimulus on a daily (DUP) or weekly (WUP) basis.
.
STUDY SHOWS: This newer study compared two different 8 week Periodization program strategies with trained males examining changes in 1RM squat, velocity/load profiles and muscular endurance. Both groups assigned loads via velocity base training at 50 to 80% of 1RM throughout the study and stopped each set at 15% velocity loss and were both matched both average in peak intensity.
.
The results showed significant differences in favor of the LINEAR programming group with 1RM squat. velocity at given loads and sub-max muscular endurance but no significant difference in countermovement jump between groups.
.
HERE’s THE REALITY: It’s pretty difficult to detect massive differences between these two groups when doing similar training programs. In Other words it’s a limited amount of time. Second, most people fail to realize is that ALL types of Periodization work. They are ALL linear over time and should be. Unfortunately the vast majority of research is comparing linear, DUP/nonlinear. There’s little Scientific research (peer-review scientific journals) on the other different and OTHER types (comparatively) such as CONJUGATE or Block style (aside from anecdotal, traditional textbook and lay articles) and that have been modified for certain sports. I am personally more of a Conjugate style fan because you can maximize & utilize a combination of all other Periodization methods.
.
Take-home message: The truth is that not a single type is the best and they all work for different types of people and have benefits.
.
. -
GET SWOLE WITH SLEEP! by Dr. Johnathan Mike
Sleep is a fascinating and complex topic that has so much individual variability yet has tremendous impact on life, stress, and physiological and psychological outcomes. For most of us, we approach and discuss sleep as if it’s only a single layer of something.
So, what is sleep really? Let’s discuss and dive deeper into sleep, science, and swoleness.
A few fun facts about sleep:
- Nathaniel Kleitman (born in 1895 in Bessarabia—now Moldova) is known as the “father of modern sleep” and earned a doctorate from the University of Chicago.
- Kleitman’s daughter (Ester) and Aserinsky in 1953 introduced the world to “rapid eye movement,” or REM sleep, making sleep a truly scientific field.
- Prior to the invention of the incandescent light bulb, we reportedly got about twelve hours of nightly sleep on average.
- Before alarm clocks were invented, there were “knocker-ups” who went tapping on client’s windows with long sticks until they were awake.
- Dogs and cats sleep over 70 percent of their lives.
- Human beings are the only mammals that willingly delay sleep.
SLEEP 101
Sleep can be defined as a reversible behavioral state in which an individual is perceptually disengaged from and unresponsive to the environment (11). It is within the Suprachiasmatic Nucleus (SCN) of the hypothalamus (the brain site of our circadian clock) that the circadian rhythm, including the sleep-wakefulness cycle, is regulated.
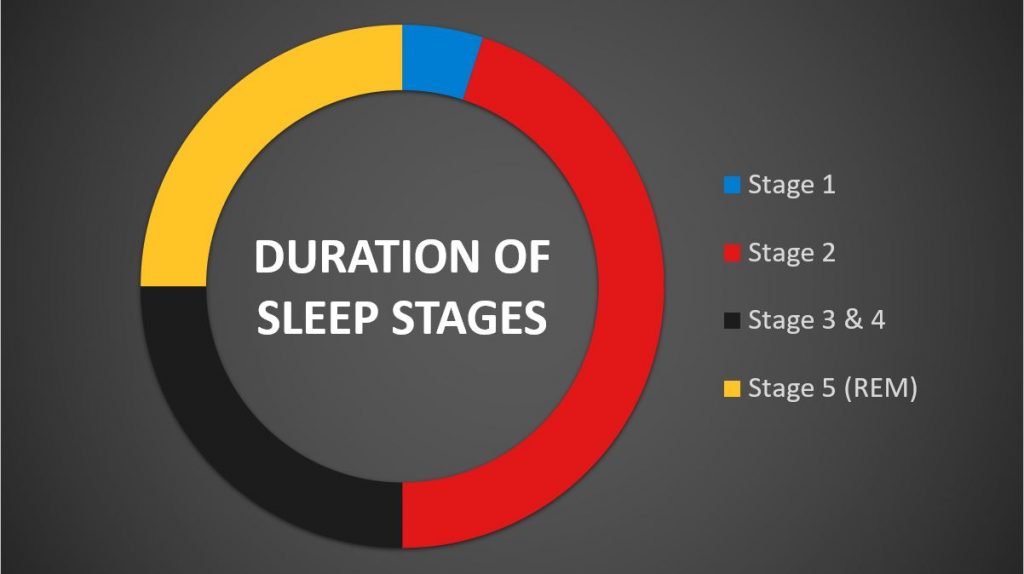
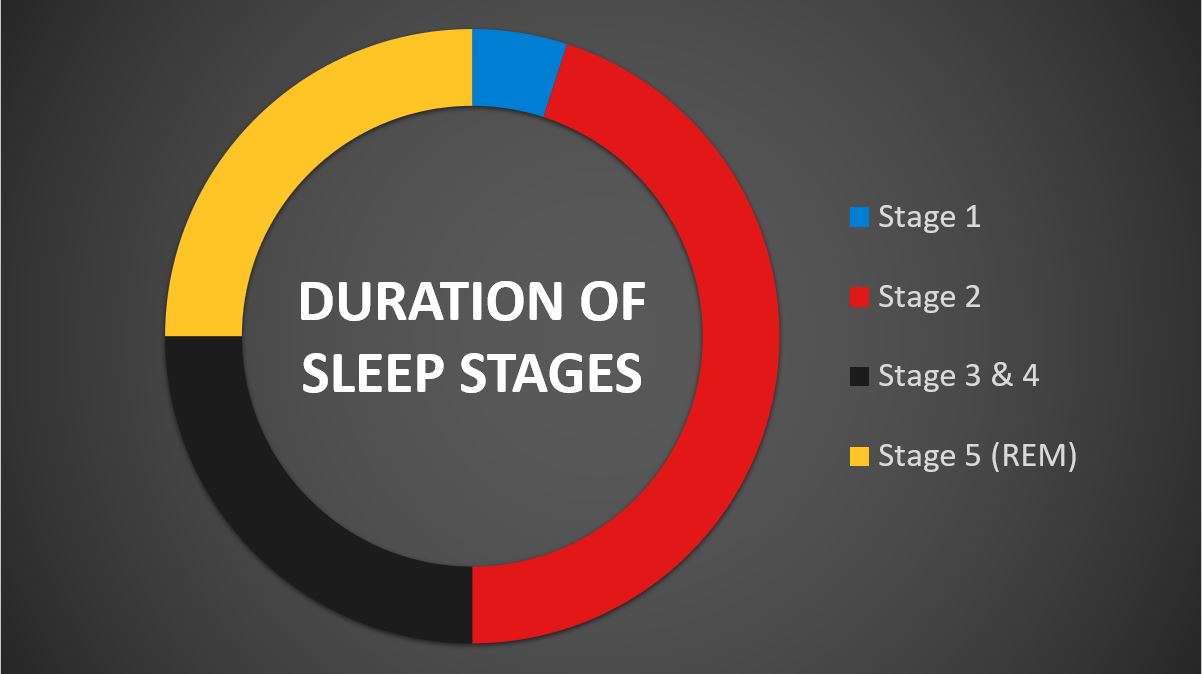
Sleep has two primary and complex physiological and behavioral states. We know these as rapid eye movement (REM) and non-rapid eye movement (NREM) sleep. NREM sleep is divided into four stages (five if you count REM) that are linked with a progressive increase in the depth of sleep (11).
Here’s another fact—the release of certain neurotransmitters (norepinephrine, serotonin, and histamine) is completely shut down during REM, which produces muscle atonia: a paralysis type of sensation during sleep), bursts of REM, and dreaming. Therefore, REM sleep is considered to be a condition with an activated brain in a paralyzed body. Very cool, isn’t it?
During the night, sleep patterns repeat intermittently, moving sequentially through four stages of non-REM sleep into REM sleep, which constitutes about 25 percent of total sleep and initially lasts approximately ten minutes and extends with each repeating cycle, lasting up to an hour in the last phase. During REM sleep, the eyes move back and forth rapidly and the body’s muscular contraction activity is minimal.
There are several stages of sleep, which has led to a whole taxonomy of sleep. It’s important to mention that beta waves are the earliest stages of sleep because you’re still awake and alert while you lay in bed watching episodes of Breaking Bad.
STAGE 1
In Stage 1,as we prepare to drift off, the brain emits alpha and theta waves. This is actually where “daydreaming” comes in, except we fall asleep. These alpha and theta waves are slower and more regular compared to the waves emitted by the part of our brain that’s awake. Individuals who practice meditation typically “hang out” in stage 1. In this stage, it’s very common to experience strange and extremely vivid sensations. One of the best examples is the feeling of falling or somebody calling your name followed by sudden muscle contractions. These are known as hypnagogic hallucinations, a collective term for sights, sounds, and other sensations experienced during the transition between wakefulness and sleep (31). Briefly following, we enter theta, which is still a relatively light period between being awake and asleep and lasts a very short period of five to ten minutes.
STAGE 2
Stage 2 lasts approximately twenty minutes, as our brain begins to generate very short periods of rapid, rhythmic brain wave activity known as sleep spindles (3). Sleep spindles are a hallmark of non-rapid eye movement (NREM). At this point, body temperature and heart rate are reduced.
STAGE 3
Stage 3 is where things start to pick up as delta waves start to emerge, which are very slow and have much larger amplitudes. Stage 3 is often referred to as delta sleep or “slow wave sleep.” Stage 3 and 4 are typically combined stages. In stage 3, it is often difficult to awaken a person, and if awakened, the person will feel disoriented for several minutes. Blood flow is directed away from the brain to other parts of the body for restorative purposes. A person can be woken up in stage 1 by a slight noise (yes, the “light sleepers”). By stage 3, he/she might sleep through a very loud bang (perhaps somebody eagerly trying to steal your protein powder). In any case, it isn’t good. Considering that sleep is vital to recovery, it is within this specific sleep stage (slow wave sleep) that growth hormone is released within humans. This has been well documented (18, 27, 33, 41, 43, 46) and suggests that optimum conditions for anabolism (aka swoleness) prevail during sleep and that the duration of slow wave sleep are proportional to preceding wakefulness (39). In addition, if/when sleep deprivation is apparent, slow wave sleep is decreased, facilitating an increase in daytime sleepiness and a reduction in performance (14).
STAGE 4
Delta sleep lasts about 25 to 30 minutes. Sleepwalking and/or bed wetting occur in this stage of sleep.
STAGE 5
The final stage of sleep is where we dream. It is actual REM sleep, lasting about 90 to 120 minutes of a night’s sleep, and is accompanied by increased respiration rate and brain activity. Herein lies a huge problem for so many individuals. If you repeatedly wake up before you get into REM sleep, you’ll begin to suffer detrimental effects to memory, motor skills, and general performance.
Dreaming occurs because of increased brain activity, but voluntary muscles become paralyzed. Although they can vary substantially, the length of a dream may last for a few seconds or as long as twenty to thirty minutes (19). Interestingly, the average person has three to five dreams per night, but some may have up to seven dreams in one night (19). These dreams can be combinations of emotion, visuals, sexual themes, black and white versus color (38), nightmares, déjà vu, or any other phenomenona. The paralyzing effect during dreams is actually a built-in protective mechanism to keep you from hurting yourself. Have you ever felt like you can’t escape during a dream? Well, it turns out you can’t. You can breathe and your basic physiology is functioning, but you really can’t move.
SLEEP, RECOVERY, AND TRAINING
Most of hard training athletes need about seven to eight and a half hours of sleep each day (2), of which 80–90 percent should be during the night. Sleep also serves as a restorative process for energy resources, tissue recovery, thermoregulation, and cognitive function (1), and deep sleep is vital for maximizing physiological growth and repair (20). Sleep is recognized as an essential component of recovery from performance training and anecdotally reported to be the single most efficacious recovery strategy. Adequate sleep is also vital for athletes who are injured, traveling, in heavy periods of training or competition phases (36, 37). Poor sleep quality, predominantly during high training loads and competition periods, has been identified as a marker of under-recovery and a contributing factor of overreaching and overtraining (13).
We all have experienced sleep disturbances the night prior to a competition, which is all too common for hard training athletes. Recent research investigated the precompetitive sleep behavior of 103 athletes and how it relates to precompetitive mood and subsequent performance (25). Results revealed that on the night before competition, athletes slept well under the recommended target of eight hours of sleep for healthy adults, with almost 70 percent of athletes experiencing poorer sleep than usual. It was found that anxiety, noise, the need to use the bathroom, and early event times were among the most commonly reported causes of disrupted sleep in athletes on the night prior to competition. Of course, disrupted sleep on the night prior to competition can negatively relate to an athlete’s precompetitive mood states. Although not conveyed in the literature, anecdotal evidence also suggests that athletes who compete at night also have complications falling asleep post-competition.
It’s been shown that hard training athletes have sleep disturbances in part related to higher nighttime epinephrine (adrenaline) and norepinephrine concentrations (30). Similarly, a doubling of training load has been reported to provoke insomnia and depression as part of the overtraining syndrome (45).

SLEEP DEPRIVATION
Sleep deprivation, sleep loss—it’s all the same. When we don’t sleep, the circadian rhythm gets off-track, hormones get crazy, and we can’t recover as effectively. Loss of sleep certainly impacts a wide variety of physiological outcomes such as altered glucose control, abnormal cortisol, and of course, overall hormonal imbalances such as lower testosterone in men (no swoleness), which impedes training recovery due to decreased protein synthesis.
There are a whole host of consequences of sleep deprivation beyond just reductions in exercise performance, both in the general populations and in athletes.
Let’s examine a variety of consequences of sleep deprivation. This, of course, isn’t an exhaustive list but highlights major components involved in sleep loss.
STRENGTH AND POWER
Blumert and colleagues (4) examined the effects of 24 hours of sleep deprivation in nine US college-level weightlifters in a randomized counterbalanced design. There weren’t any differences in any of the performance tasks (snatch, clean and jerk, front squat, and total volume load and training intensity) following 24 hours of sleep deprivation when compared with no sleep deprivation (4). However, mood state, as assessed by the profile of mood states (a questionnaire used for overtraining), was significantly altered with confusion, vigor, fatigue, and total mood disturbance all negatively impacted by sleep deprivation. There have also been performance declines in isokinetic knee extension and flexion torque after thirty hours of sleep deprivation in trained men (9). An early study also found a significant effect of sleep loss on maximal bench press, leg press, and deadlifts but not maximal bicep curls. Submaximal performance was significantly negatively affected on all four tasks and to a greater extent compared to the maximal efforts (34).
Bottom line on strength and power: In all likelihood, sleep loss will affect your gains, but individual variability does exist as well as differences in training responses and programs.
HORMONES
Testosterone is also affected by your total amount of sleep. This makes sense, as our bodies make much more testosterone when we’re asleep than when we’re awake. A lack of sleep can most certainly create a decrease in testosterone. A recent investigation found that men who slept less than five hours a night for one week in a laboratory had significantly lower levels of testosterone (by over 10 percent) than when they had a full night’s sleep (26) whereas an early report showed a 30.4 percent decrease (12). Interestingly, these reductions all happened within 24 hours of sleep deprivation (13, 17).
In a study by Leproult and colleagues (26), the participants spent three nights in the laboratory sleeping for up to ten hours and then eight consecutive nights sleeping less than five hours. Their blood was sampled every 15 to thirty minutes for 24 hours during the last day of the ten-hour sleep phase and the last day of the five-hour sleep phase. The results showed that sleep loss on testosterone levels were apparent after just one week of decreased sleep, and five hours of sleep decreased their testosterone levels by ten to fifteen percent. It was also found the men had the lowest testosterone levels in the afternoons on their sleep restricted days, between 2:00 p.m. and 10:00 p.m., and also self-reported their mood and vigor levels throughout the study. In addition, the young men reported a decline in their sense of wellbeing as their blood testosterone levels reduced. Their mood and vigor actually decreased more per day as the sleep restriction part of the study continued.
Growth hormones are secreted in a pulsatile fashion from the anterior pituitary shortly after sleep. As previously mentioned, growth hormone is well documented for promoting anabolic effects during sleep. However, considerable sleep deprivation for multiple nights can undoubtedly crush growth hormone. But some evidence indicates that neither an irregular sleep cycle [i.e. night shift workers (7)] nor only sleeping for four hours a night (41) will adversely affect whole-day exposure to growth hormone. Although sleep loss can disturb changes in the growth hormone cycle, overall exposure is still present, as the body appears to compensate during normal waking hours.
Cortisol is a steroid hormone that is produced in the adrenal cortex located on top of each kidney. Cortisol is released in a highly irregular manner with peak secretion in the early morning, which then tapers out in the late afternoon and evening. Fasting, food intake, exercising, awakening, and psychosocial stressors cause the body to release cortisol, but it has a slightly different response when sleep loss is apparent. The majority of the recent science on cortisol and sleep deprivation shows either no change or slight increases. Some studies even normalize this difference and increase overall exposure to cortisol over a full day.
Similar to cortisol, insulin doesn’t appear to be highly disastrous to sleep loss (unless you eat a large meat-lovers pizza with everything drizzled in olive oil right before your four hours of sleep). However, some evidence does show a decrease in insulin sensitivity in the fat cells and liver (8, 15). Some evidence reports that this decrease in insulin sensitivity can be attributed to getting half your normal amount of sleep for less than a week (10, 35).
Bottom line with sleep and hormones: Try not to screw them up! For those of you who are ramping up training efforts for competition, you may want to get more total hours on the pillow.
METABOLISM
Studies support the notion that chronic partial sleep loss can increase the risk of obesity and diabetes (24). This includes changes in glucose regulation via insulin resistance, deregulation of neuroendocrine control of appetite, and/or increased energy intake (1, 40). Sleep deprivation has also been shown to have decreases in leptin and increases in ghrelin [appetite regulating hormones (47)]. Sleep loss has also been shown to increase hunger and appetite, particularly in relation to carbohydrate-rich foods (42). Metabolic rate itself is a bit mixed. One study found that getting three fewer hours of sleep per day for two weeks resulted in a 7.6 percent reduction in metabolic rate (29) whereas other reports showed no decrease (6, 32). To add to the mix, a recent study in adolescent boys reported that less sleep actually resulted in additional calories expended (23), meaning the subjects expended more (being awake longer) and consumed less (decreased appetite).
Bottom line with metabolism: Altered glucose metabolism and neuroendocrine function can create concern regarding carbohydrate metabolism, appetite, food intake, and protein synthesis.
COGNITION
There isn’t any doubt that one of the most studied areas of the science of sleep deprivation is the effects on alertness and performance (44). It is estimated that the consequences cost billions of dollars worldwide per year due to accidents, direct healthcare costs, and reduced efficiency and productivity (44). Sleep loss surely decreases the effects of learning and memory and is critical for learning and preparing the brain for next-day memory development (48). Interestingly, a recent study found that 24 hours of sleep deprivation significantly heightened the levels of stress hormones and lowered attention and working memory. This means that the acute loss in sleep rendered the subjects more susceptible to making errors despite the fact that they were all good sleepers, had no history of medical or neuropsychiatric diseases, weren’t taking any kind of medication, and were in their early to mid 20s (22). Although a lack of overall evidence exists on the effects of sleep deprivation risk of acute injury (i.e. decreased focus, poor execution, or lowered reaction times), it’s likely that sleep deprivation may increase susceptibility to injury.
Bottom line on cognition: Sleep loss can negatively impact learning, memory and likely increase the risk of injury and work related errors.
IMMUNE RESPONSE AND INFLAMMATION
Ever have the feeling of sickness and headaches due to loss of sleep? Say I! Well, a recent review examined the link between sleep and immune response and concluded that sleep improves immune responses and that most immune cells have their peak pro-inflammatory activity at night (5). This means that sleep loss will certainly impair immune responses, increasing risk of illness. A recent study examined immune function response in subjects who naturally slept for less than seven hours, seven to nine hours, or longer than nine hours (16). Short sleep duration was associated with 49 percent higher T-cell function in response to an antigen and 30 percent lower natural killer cell activity when compared with normal sleep. Simply put, sleep loss lowers immune function.
Inflammatory markers are also present with sleep deprivation. Interleukins (naturally occurring proteins produced by the body that have infection-fighting immune responses), tumor necrosis factor-α (important mediator of the body’s response to infection), and C-reactive protein (a substance produced by the liver that increases in the presence of inflammation in the body) are all influenced by a lack of sleep (28) as well as gender differences (21). Those people with insomnia and sleep apnea have elevated inflammatory markers (28), which absolutely affect insulin sensitivity, metabolism, blood pressure, and sleep.
Bottom line on immune response and inflammation: Loss of sleep does decrease immune function and can adversely affect performance whereas additional and consistent sleep surely helps reverse the process.
Download the references and additional resources: references-sleep-to-swoleness-dr.-j-mike



{kind=link}